



Viruses and cancer cells, casual friends looking for antibodies
For infections, cancer, autoimmune diseases. Antibody-based therapies have been on the rise in recent years. But how do you find the antibodies that will be used in hospitals? Although it may be rare, the response is related to cancer cells and viruses.
What and how are antibodies?
Antibodies are one of the cornerstones of our body’s defenses; they recognize the intruder and mark the immune system to suppress it. In addition to recognizing viruses, bacteria and other infectious agents, they are also able to target the immune system against cancer cells. Or, if they bind to healthy cell structures, they can damage them, leading to the development of autoimmune diseases.
B lymphocytes secrete antibodies when they detect something they don’t know, called an antigen. B lymphocytes can produce antibodies against a wide variety of antigens—we have the possibility of producing a billion different ones!—where each type of B cell or clone recognizes a specific antigen. Each B cell clone produces a single class of antibodies, called monoclonal antibodies1.
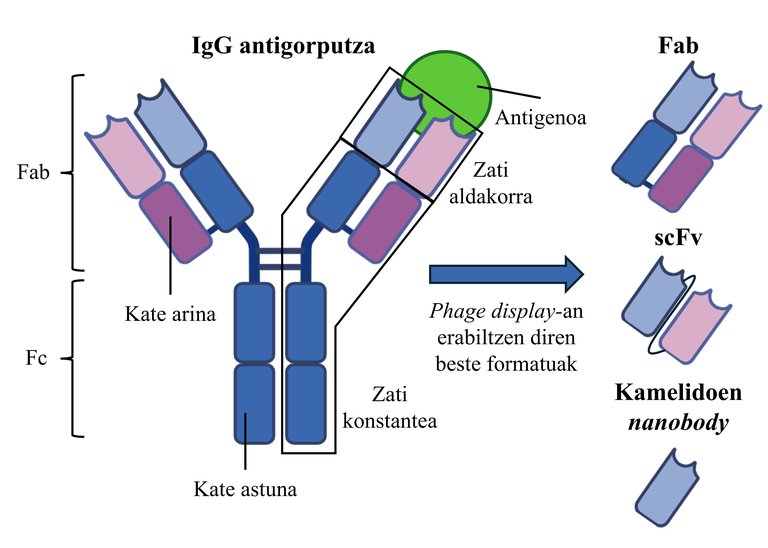
Structurally, antibodies are composed of two identical units, two monomers, each containing two chains: the short light chain and the long heavy chain. Functionally, we can divide these proteins into two parts. In one aspect, there is the antigen-specific binding portion, referred to as the Fab (antigen-binding fragment). The Fc part (fragment crystallizable) is associated with other elements of the immune system to elicit an immune response2 (Figure 1).
The world of immunotherapy
Suppose someone is unable to produce a strong immune response on their own, or is at risk of being in contact with a pathogen. These people can be administered monoclonal antibodies directly through the blood to quickly carry out the immune response, activate or block the different pathways of the immune system... depending on the needs of the patient. That's what immunotherapy is all about. Currently, immunotherapy against cancer stands out, with 46% of the antibodies used in the clinic. However, antibodies for the treatment of immune-related diseases are also abundant, 27%. They are also used to treat infectious or cardiovascular diseases, including3 (Figure 1).
Since monoclonal antibodies are useful for a variety of conditions, it is not surprising that they have aroused the interest of the pharmaceutical industry. In fact, although it is not a new therapy, they are among the most widely used drugs on the market4 in recent years. Therefore, the discovery of new antibodies is in full actuality. But how are they looking?
Looking for antibodies
The first of the antibody discovery techniques is the hybridoma technology (Figure 2). georges JF was founded in 1975. Researchers Kohler and Cesar Milstein, and for the time being most of the antibodies used in hospitals, have been discovered by this method. In this technique, laboratory animals, particularly mice, are immunized with the antigen of interest to elicit an immune response against it (Figure 2A-1. Step 2). The animal's spleen is then harvested and the active B lymphocytes present therein, i.e., antibody-producing cells, are isolated (Figure 2A-2. Step 2). B lymphocytes are then cultured in the laboratory together with myeloma cells which, in the presence of cancer cells, allow continuous growth. Due to cell culture conditions, fusión between myeloma cells and B lymphocytes is enhanced by forming so-called hybridoma cells (Figure 2A-3. Pause). Each hybridoma will produce a single type of antibody. Finally, the hybridomas that synthesize the antibodies that best recognize the antigen5 will be selected (Figure 2A-4. Step 2).
But the method has several disadvantages. For example, that the antibodies produced are of mouse origin. Therefore, strategies have been sought to humanize these antibodies, such as the use of transgenic mice with a humanized immune system6. In any case, the process of producing hybridomas is long and very low in yield, where only 1% of the hybridomas will survive5. With limitations and an ethical approach, methods were created that prevent the use of laboratory animals. Among them, the most notable is the one based on the presentation of the large collection of antibodies on the surface of viruses: phage display (Figure 2).
The virus presents antibodies
Phage display technology is not new, as it dates back to the 1980s. The core of this technique is the bacteriophage M13, a virus that infects bacteria. This phage has a protein called pIII on its surface. If we associate the gene of a protein of interest with the gene of that protein, pIII and our protein will be expressed together without adversely affecting their ability to be infected on the outside of the virus. Therefore, we can create a collection of phages that present different antibodies, from which we will select those capable of detecting the target of our interest, the antigen. Where did these antibodies come from?
Sources of antibody libraries
One of the strategies is based on people immunized with a particular antigen, such as those who have had COVID-19 or have been vaccinated. Once an anti-antigen response has been generated, collect the activated B cells (Fig. 2B - 1. step) from a blood sample, and the specific sequence of the monoclonal antibody produced by each clone is acquired by PCR. All sequences are then randomly joined to the pIII protein gene with one pIII-antibody molecule per antibody sequence. Finally, the collection of pIII-antibody sequences is included within the bacteria along with the other genes necessary for phage production; that is, we “artificially infect” the bacteria. The "infected" bacteria will then produce phages with a known pIII-antibody on their surface (Figure 2B - 2. Step 2). This type of antibody library is called an immune library, and for each antigen of interest a library is formed1,6.
In contrast to libraries produced against a specific antigen, naïve libraries are produced from healthy or non-diseased human B lymphocytes. That is, in this type of library the immune response to a single antigen does not predominate, they are more versatile1,6. In any case, precisely because a response to a specific antigen has not developed, antibodies obtained from naïve libraries generally have a lower affinity than those obtained from immune libraries. Affinity enhancement strategies are then used8.
The more diverse the antibody library is, the more likely it is to find an anti-antigen of interest. Synthetic libraries were created with this idea. In this case, the number of monoclonal antibody types in a library is artificially increased. To do this, the sequences of the areas responsible for antigen recognition are modified in the laboratory randomly or to meet specific characteristics and antibodies that do not exist naturally6 can be obtained.
In either case, the antibodies are presented on the surface of the phage. The phage library is contacted with the target antigen and the phages that remain bound thereto are selected (Figure 2B - 3. Step 2). This process is repeated three or four times, placing increasingly stringent conditions for addition. This allows the identification of specific antibodies with only a high affinity for the antigen, which best recognizes the antigen (Figure 2B - 4. Step 1,2,6,7.
An antibody, eleven forms
When we think of antibodies, we usually think of Y-shaped proteins. And while this is true for most human antibodies, such as IgG (Figure 1), these molecules are too complex to display on the surface of phages. This is because phage producing bacteria cannot produce complex molecules such as IgGs. Therefore, only some IgG fragments are used in the phage display. One of them is the part that recognizes the antigen, i.e. the Fab. The Fabs are composed of two chains, each chain having a constant part and a variable part (Figure 1). But to facilitate the production of antibody libraries, single-chain formats have been obtained. The most commonly used among them are the so-called single-chain fragment variable (scFv), in which the variable parts of the two chains are joined1,9,10 (Figure 1). However, many other formats are used, such as small and rare antibody fragments obtained from camelids, nanobodies 11.
Beyond phage display
Phage display technology has certain limitations that can lead to the failure of some of the selected antibodies. In one aspect, the process typically begins with working on scFv or Fab formats, which are produced in bacteria. But antibodies are commonly used in the clinic in the form of IgG; they are those produced in mammalian cells. Therefore, it is necessary to change the format and mode of production, which may be detrimental to the structure and characteristics of antibodies.
It has been proposed to replace phages with more complex organisms, such as yeasts (yeast display), capable of presenting IgGs in their entirety. However, compared to phage display, the performance of the process is lower and antibody libraries are less diverse12. Alternatively, mammalian cells (mammalian display) may be used directly. But while collections of suitable IgG-presenting cells can be completed, the current ones are small and the process for doing so is very expensive and difficult12.
On the other hand, the ability to recognize antigen only in phage display is taken into account when selecting antibodies without taking into account other characteristics such as stability13. In recent years, many computer tools have been created to predict antibody characteristics. Therefore, they can help to select the most suitable antibodies14.
Therefore, although viruses and cancer cells have always been considered enemies, for 40 years they have been indispensable collaborators in the search for new antibodies.
Bibliography
1. Nur A. Et al. 2023. Antibody Phage Display. Phage display: Methods and Protocols, Springer US, New York, NY.
2. Lu R.M. Et al. 2020. "Development of therapeutic antibodies for the treatment of diseases". J. J. Biomed Sci. Sci. 27 1.
3. YAbS. https://db.antibodysociety.org/
4. Antibody Therapy Market Size, Growth Analysis 2023-2032. Global Market Insights Inc. https://www.gminsights.com/industry-analysis/antibody-therapy-market.
5. Mitra S. and Tomar P.C. 2021. "Hybridoma technology; advancements, clinical significance, and future aspects." J. J. Genet Eng Biotechnol. 19, 159.
6. Geyer C.R., McCafferty J Dübel S., Bradbury A.R.M. and Sidhu S.S. 2012. "Recombinant Antibodies and In Vitro Selection Technologies." Antibody Methods and Protocols, Humana Press, Totowa, NJ.
7. Zhang Y. 2023. "Evolution of phage display libraries for therapeutic antibody discovery". MAbs 15, 2213793.
8. Lim C.C., Choong Y.S. and Lim T.S. 2019. "Cognizance of Molecular Methods for the Generation of Mutagenic Phage Display Antibody Libraries for Affinity Maturation". INT. J. J. Mol Sci. Sci. 20, 1861.
9. Huston J.S. Et al. 1988. "Protein engineering of antibody binding sites: recovery of specific activity in an anti-digoxin single-chain Fv analogue produced in Escherichia coli". Proc Natl Ed. Ed. Sci. Sci. U. U. S. S. A. A. 85, 5879–5883.
10. Bates A and Power C A. 2019. "David vs. Goliath: The Structure, Function, and Clinical Prospects of Antibody Fragments". Antibodies 8, 28.
11. Khodabakhsh F., Behdani M., Rami A. and Kazemi-Lomedasht F. 2018. "Single-Domain Antibodies or Nanobodies: A Class of Next-Generation Antibodies. INT. Rev. Immunol 37, 316–322.
12. Slavny P. et al. 2024. "Advances in mammalian display technology for therapeutic antibody development and beyond: current landscape, challenges, and future prospects." Front Immunol 15, 1469329.
13. Kasana A., Kapoor K. and Verma V. 2025. "From Phage Surface to Bedside: Development of Therapeutic Monoclonal Antibodies using Phage Display". Curr Pharmacol. Rep. 11, 54.
14. Zheng J., Wang Y., Liang Q., Cui L. and Wang L. 2024. The Application of Machine Learning on Antibody Discovery and Optimization. Molecules 29, 5923.
Buletina
Bidali zure helbide elektronikoa eta jaso asteroko buletina zure sarrera-ontzian







