



Laryngectomy: Recovering Voice
Primary phonatory fistuloplasties
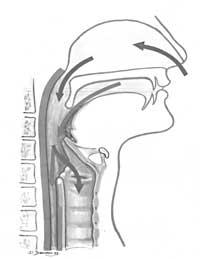
In this type of cut the laryngectomy is performed simultaneously with voice recovery.
PARDIWALA mentions among other conditions for performing primary phonological fistuloplasty:
- Complete tumor eradication is an indispensable condition.
- Do not excessively increase mortality and morbidity.
- Do not make swallowing difficult.
- Get a good voice.
For us there are also four predominant ideas when performing primary phonological fistuloplasty.
BLOM and SINGER said an internal fistula without a device had to be achieved. Due to the techniques of the time there were many problems, such as fluid and solid output and fistula obstruction. Therefore, many reviews had to be made. Surgeons should choose between primary and secondary phonological fistuloplasty. We are supporters of primary phonological fistuloplasties, because the disease begins to speak quickly. However, the favorable and contrary reasons for primary phonological fistuloplasty depend on several factors.
a) Local factors
Tumor location
When primary phonological fistuloplasty is proposed, oncological treatment is essential, i.e. the tumor must be completely removed.
Laterocervical adenopathies
In general, the appearance of adenopathies will not alter our surgical criteria. Any fistuloplasty technique should allow the emptying of the cervical lymph nodes for their oncological acceptance.
Previous irradiation
Irradiation prior to laryngectomy does not imply the inability to use this type of surgery
...b) General factors
Metastasis
When there is metastasis in the body, we will follow the criteria used in any laryngeal surgery. In these cases we do not do any primary fistuloplasty.
Bad general status
The general poor state does not prevent total laryngectomy, but in this situation fistuloplasties are not performed simultaneously.
Age
We do not believe there is an age limit for this type of cut. We all know that there are 70-year-old people who are well physically and psychically, while 50-year-old others are in bad shape.
Gender
When performing a total laryngectomy for women, their mood, social status, age, and other factors will be considered below.

Pulmonary status
Anyone who is going to have a total laryngectomy should have a respiratory status study, but in case of simultaneous fistuloplasty, the test should be deeper.
;breathing to perform fistuloplasty should be in good condition.Cardiac Situation
The heart condition does not prevent fistuloplasty by itself, as long as it does not prevent total laryngectomy.
Intellectual level
The intellectual level cannot be considered an absolute conditioning, but the minimum level of intelligence is necessary to understand the new anatomical situation. Sometimes, along with the low intellectual level there are other negative factors such as social, labor, motivational, etc. Some patients should be excluded from this situation.
Social level
This factor is also not decisive. The results obtained are better than in the case of high-level professionals such as engineers or architects.
Motivation
The patient's motivation to continue speaking is very important for the success of the surgical technique.
Family atmosphere
This factor is closely related to the previous ones. The family in general, and the couple in particular, will have great influence on the final results.
Motor status
The patient's ability in the hand is critical for plugging the tracheostomy with the finger or for placing or removing the fonatorium prosthesis and valve. Therefore, lack of motor coordination, vibrations, parkinson, arthrosis in hand, etc. This type of cut is not possible for those who have.
Psychic Situation
These techniques are not applicable to patients with psychic or psychiatric problems for any reason, such as alcohol.
Secondary phonological fistuloplasties
This name indicates the cut for patients who have had a laryngectomy to recover their voice.
SPOFFORD, JAFEK and BARCZ cite four conditions to use the tracheal puncture technique in fistuloplasties:
- Safety and absence of undesirable esophageal perforations.
- Speed and ease.
- In external consultations and local anesthesia.
- Make cutting equipment simple and economical.
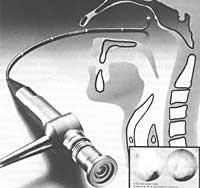
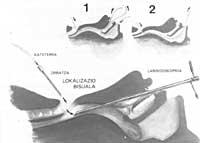
Secondary fistuloplasties can be classified into two techniques: tracheal puncture technique and tracheal ascension technique.
Some local and general factors should be taken into account in secondary fistuloplasty.
a) General factors
Despite taking into account here the factors mentioned in primary phonological fistuloplasties, there are three other factors to be analyzed.
Phonological status of the patient
The social reinsertion of the patient will depend on the level and quality of the voice achieved. Therefore, secondary fistuloplasty techniques will be used in the following patients:
- Although they try it completely in patients who have not reached the erygmophonic voice.
- Patients who have not reached the erygmophonic voice due to psychological problems.
- Despite being an erygmophonic voice, in patients who because of their poor presence want to improve their voice.
- Patients with a good erygmophonic voice who for work needs want to improve their voice.
- In those who use electrolarynx but do not correspond to the voice obtained.
- Patients who by their voice have not been able to develop in society, family or work.
Phoniatric control
Although the control of the phoniatrist can improve the quality of the voice, it does not seem essential to us. The patient normally leaves the hospital speaking and only he learns to improve his new voice.
Language mobility
In all cases where secondary phonological fistuloplasty is required, the state of the mobility of the tongue should be analyzed, since for a good use of the fistula the mobility of the tongue should be normal. Although it is not frequent, laryngectomy can cause damage to the hypoglossal nerves that can hinder the mobility of the tongue.
b) Local factors
Local cancer situation
Thereafter there will be no risk of renewal.
State of the neck by irradiation
A patient who has not undergone irradiation to apply any fistuloplasti technique is in much more favorable conditions than another who has suffered, since the healing will be much better and the fistulas will not tend to close or open.
Anatomical condition of the neck
In general, the anatomical state of the neck should not be an obstacle to fistuloplasty.
Tracheostomy status
For the application of any secondary technique it is convenient that the tracheoostoma is not submerged behind the breastbone. In these cases, if other conditions are met, we prefer to make the tracheal ascent.
Size of tracheostoma
If traqueostomas are small and other conditions are met, we prefer to do the tracheal ascent.
Excessively large tracheostomas are also not suitable for secondary fistuloplasty by puncture, since although there are no problems to apply this technique, tracheostoma cannot be completely covered with the finger, so the air escapes worsening the fonation.
Patients who have not lost cricoid when performing laryngectomy
Tracheal puncture cannot be performed in cricoid patients. You have to remove the cricoid and at the same time we do the tracheal ascent.
Tracheoesophageal wall
We consider it important to know the thickness of the tracheoesophageal wall to apply one or another technique.
If the thickness is two or more centimeters, the tracheal puncture does not seem appropriate. After tracheal puncture, the wall thickens more and the prostheses to be used are long, so they lose almost all the characteristics of the fonation.
State of the pharyngoesophageal part
In the fistula area there should be no stenosis and the hypolarynx should be wide and adequate.
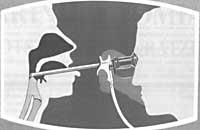
Faringo-esophageal insufflation test (AIR BLOWING TEST)
This test leads to the esophagus and checks if the patient speaks. If the patient speaks, the outcome of the surgical technique is expected to be satisfactory.
SINGER and BLOM attach great importance to the preoperative test to predict successes or failures. However, for us the results of this test are variable and have no total reliability.
Pharyngo-esophageal pressures
It is the normal physiologism of the pharyngo-esophageal part, one of the most important conditions for the development of a good voice erigmophonic and the acquisition of a new voice after fistuloplasty.
Type of secondary technique
In the case of secondary phonological fistuloplasty, together with the factors analyzed so far, the need to place prostheses on a patient should be assessed. The patient to whom the prosthesis is applied should be very careful with the prosthesis, as it will create a lifelong servitude. The existence of prostheses entails a constant economic cost and some of them involve problems of adaptation.
In case of tracheal puncture, the patient must carry the prosthesis constantly 24 hours a day, since the fistula can be closed in a few hours without prosthesis.
Therefore, you have to choose the puncture or ascent for each patient.
Anesthesia
The type of anesthesia to be used may condition the choice of the surgical technique. Since patients with good general condition may have any type of anesthesia, the factors analyzed so far will be applied.
We try to perform a tracheal puncture, which can be performed under local anesthesia, for those people who due to their general poor condition cannot be subjected to general anesthesia and who may suffer secondary phonological fistuloplasty.
Therefore, each reader, each patient must be analyzed accurately so that the decision is correct, but after the intervention phoniatric rehabilitation will be very important. According to CONLEY, 40% of patients reject phoniatric rehabilitation, giving up the therapist's advice.
Translation: J. Related information
Buletina
Bidali zure helbide elektronikoa eta jaso asteroko buletina zure sarrera-ontzian







