



Computer diagnosis: medical computers
OBD systems: What and for what?

The appearance of all these techniques helps doctors diagnose and cure diseases. However, we must not forget that these images only show a part of reality and that their interpretation is essential. In fact, interpretation is a critical step in diagnostic imaging and physician preparation and experience are of vital importance.
A computer diagnostic system (OBD) aims to help the doctor - usually radiologist - interpret radiological images. Research on these systems originated in the 1960s, but now is the time when more momentum is taking place. In general, the development of an OBD system requires the participation of a multidisciplinary team, since artificial intelligence principles are used to answer biological questions through the processing of digital images.
It is often used to detect tumors of any type. For example, they can help diagnose breast cancer in a mammogram or look for millimetric lung tumors in a CT image. We will take this last example to see in more detail the utility of a BOD.

A current pulmonary CT figure shows the morphology of this organ with an approximate accuracy of one millimeter. This high accuracy implies a large size of the images. It is not uncommon to get around 400 axial cuts (which separate the body from the head to the legs) of 512x512 pixels per scanner. Each of these 400 images has a lung section, usually one millimeter thick.
If the radiologist wants to look for a tumor in this large dataset, he or she should observe one by one the 400 sections in search of a spherical object of a few millimeters. A hard work, hard and of great responsibility, certainly. Therefore, any radiologist dreams of a computer program that would allow him to read the complete image and, in case of any tumor, locate it and size it in a few minutes. Well, many groups of scientists are working in the world to realize this dream and the goal is not so far. But how can you get something like that?
Operation of OBD systems

Preprocessing
The aim of this step is to adapt the image characteristics for the following tasks. For example, filters can be applied to reduce image background noise or reduce size (number of pixels) to reduce the complexity of the algorithms to be applied later.
Segmentation of the areas to be analyzed
Before going to specific studies it is necessary to divide the image into several sections. For example, in order for the OBD system to look for tumors in the lungs, you should first find lungs. Segmentation strategies are diverse and published monthly in specialized journals such as the IEEE Transactions on Medical Imaging.
One technique or another is used depending on the characteristics of the image and the part that you want to segment. If the contrast between the part we want to separate and the rest of the image is large, as usual in lung images, we can base ourselves on the intensity of the pixels to perform segmentation. Thus, as the air appears darker than the body's materials, this information will be used to separate the lungs.
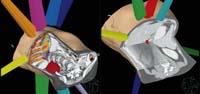
Conversely, the prostate and other similar organs are found among similar tissues. Segmentation of the prostate is now a mandatory step in radiotherapy planning. In these cases, rather than based on pixel intensity, the program can 'learn' the forms and possible locations of the prostate from previously segmented images. This set of images that will serve as reference are called atlas. In this way, the BOD will try to adapt those forms and locations studied to the new image and as a result will offer the doctor a segmentation of the prostate. This proposal may not be completely correct, so normally the doctor can correct it manually.
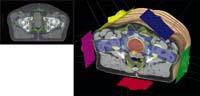
As can be seen with these two examples, segmentation is not a simple task and should be adjusted to each application. It is often impossible to develop fully automatic systems, and user participation is often necessary.
Classification and evaluation
This last step also depends on the requirements of each BOD. In general, the final results will be the nature, location and size of the pathology sought. For example, in the case of the aforementioned lung tumor detection program, the results of this step would be the location and size of the tumors. In the case of interpretation of mammograms, on the contrary, the program would mark areas potentially affected by cancer. Advanced artificial intelligence techniques are used to perform this work.
In short, the BOD analyzes the segmented image part in the second step, in search of areas with differential characteristics of certain pathologies. These differential characteristics are defined directly and indirectly.

The transversal option is based on the principles of artificial intelligence. In short, it is about computers learning for themselves using examples. For example, we may have hundreds of different lung tumors to the computer and other parts of the lung that are not tumors. The BOD will analyze the characteristics of all these sections, such as intensity, partial derivatives, compactness, structure, etc. And finally, it will create rules to classify parts of the image based on all these characteristics and to determine whether or not they are tumors. That is, you will use our examples as training to learn the characteristics of tumors.

This last step is of vital importance as the difference between the detection or not of a tumor is very large. With current techniques it is impossible to achieve 100% accuracy. The main problem is that the degree of sensitivity and specificity cannot be simultaneously very high. Sensitivity is the probability of finding them if tumors exist, while specificity is the probability of correctly classifying nontumor. When seeking greater sensitivity, the number of false positives necessarily increases. Consequently, there is currently no fully autonomous BOD and all systems used must be supervised by a physician.
DBO in reality: will it be useful?
The first DOBs used in hospitals worldwide were mammography interpretation assistance systems, since they were officially recognized in the US in 1998. Since then they have been used mainly in the USA and Holland. They are used to issue a second opinion, that is, instead of replacing the doctor, they offer a second opinion.
According to studies prior to official approval, these software reduced the percentage of tumors not detected in mammograms. However, according to a study published in April 2007 in the prestigious journal The New England Journal of Medicine, this improvement is not remarkable at all. The researchers analyzed the cases of 222,135 women who went to perform mammograms in the US between 1998 and 2002. In cases where the OBD system was used, 32% more women called for a second study and 20% more had a breast biopsy. However, for each tumor discovered by OBD, there were 2,000 false positives. As the researchers indicate in the conclusions of the article, BOD considerably reduces the degree of accuracy in the interpretation of mammograms and the increase in the number of biopsies is not associated with a higher degree of tumor detection.
The net results of the aforementioned article have cooled the optimism about OVDs. It is clear that these systems can be of great help, but before their implementation in hospitals it is necessary to demonstrate their usefulness through reliable research.
In addition to OBDs for interpretation of mammograms, the US Government has authorized software for the study of lung tumors in recent months, always in order to use these software to issue a second opinion. That is, OBDs continue to work as 'helpers' and in no case are they able to replace the doctor.

But will they be able to do so in the future? The development experienced in this field in recent years and the high number of researchers in the world allow to predict a rapid development of computer diagnosis, and it is possible that these systems can respond to medical work in certain tasks ahead of schedule. However, initially they will only be used for very specific tasks and always under medical supervision. As the technique progresses, they will be able to take on increasingly complex tasks with less supervision. Doctors may be calm, but they won't lose work. And it is that nobody would feel comfortable if when going to the doctor found a computer screen instead of a person with white apron.
Buletina
Bidali zure helbide elektronikoa eta jaso asteroko buletina zure sarrera-ontzian










