



Is cholesterol so bad?
This knowledge, however, is often incorrect and the bad prestige of cholesterol is very widespread. There are those who think it is a disease! It must be made clear, however, that cholesterol is not harmful in itself, but is synthesized in the body of animals and is essential for life.
What is cholesterol?

Cholesterol is an alcohol from the steroid group. Although it differs much from other lipids, it is classified among them because it dissolves only in organic solvents, that is, it does not dissolve in the blood, which is very important to understand how it is transported by the body.
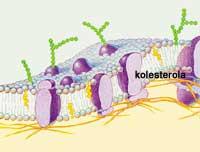
Cholesterol XVIII. It was first isolated in the nineteenth century and appears in the nature of two forms: free or sternal, united to different fatty acids. It is present in all vertebrate and invertebrate animals, constituting the basic component of the cell membrane and giving stability to the membrane, especially before temperature changes. In addition, it protects and isolates the nerves. In mammals, cholesterol is more abundant in the brain, liver, skin, and adrenal glands.
It is also a precursor to many other steroids with important metabolic functions. From cholesterol are synthesized vitamin D, bile salts that help digestion and steroid hormones: glucocorticoids, mineralocorticoids and sex hormones, both female (estrone, estradiol and estriola) and male (androsterone and testosterone).
On the other hand, the body has two sources of cholesterol: the first is endogenous, that is, produced in it, especially in the liver; the second is exogenous and penetrates the body through food. Taking into account the dietary habits of developed countries, about 85% of the total cholesterol is produced in the body itself. It is generated in the mitochondria of hepatic cells (approximately one gram per day) and among the enzymes involved in the synthesis is the reduction B-hydroxymethylglytaryl CoA. This enzyme is the key to synthesis reactions and some drugs deactivate this enzyme and lower blood cholesterol.
In fact, many epidemiological studies relate the presence of high levels of cholesterol in the blood with arteriosclerosis, and although cholesterol is not the only explanatory agent of this disease, it seems that this (or more directly one of the lipoproteins that carries it) is the main culprit.
Transportation of blood cholesterol
Cholesterol is generated and stored in the liver and reaches all other tissues of the body through blood circulation. For this purpose, it needs transporting lipoproteins that do not dissolve in aqueous solution.
Lipoproteins are spherical particles, formed inside by a lipid core that contains the esters of cholesterol and triglycerides, and in the outer layer are phospholipids and water-soluble apoproteins. Through apoproteins they bind to cell receptors and each type of lipoproteins has their own special apoproteins. Other features that are taken into account when characterizing lipoproteins are the size, density, or lipids they carry.
Thus, they are classified in five types: kilomicrons, very low density lipoproteins or VLDL ( very low denity lipoprotein ), of medium density or ILDL ( intermediate denity lippoprotein ), of low density or LDL ( low denity lipoprotein ) and of high density or HDL ( high denlipoprotity ). Although the km and VLDL transport mainly triglycerides, all carry cholesterol. However, it is not a very fast transport, as it moves less than 1-2 grams of cholesterol a day.
Evolution of food and production
The average daily intake of cholesterol is 250-500 mg. After eating a food containing cholesterol, the intestinal cells absorb 40% of the cholesterol. This cholesterol, along with triglycerides, is concentrated in kilometres. These large low-density lipoproteins penetrate the blood circulation and when reaching the muscles and fatty tissues release triglycerides. This allows the muscles to acquire energy and that in the fatty tissues they accumulate reserve fats. Once the triglycerides are distributed and when they hardly have cholesterol esters, the remains of kilomicrons go to the liver.
In liver cells, special receptors identify these residues and insert them into the cells. However, the cells do not consume all the cholesterol, part of what is left is excreted into bile acids and part is free in the blood. Blood cholesterol can be reabsorbed in the intestine and returned to the cycle. Therefore, the cholesterol that is introduced with food makes the way between the intestine and the liver. In addition, a little cholesterol is lost through the excrements.
The cycle of cholesterol that produces the body is different. The cycle begins in the liver cells, where cholesterol is produced. Then, along with triglycerides, it passes to the blood united to lipoproteins VLDL. VLDL, like the kilomicrons, release triglycerides in the muscles and fatty tissues. As proteins and lipids are lost, they become medium density lipoproteins (IDL), low (LDL) or high (HDL), respectively.
Cholesterol ‘good’ and ‘bad’
Approximately 75% of the total cholesterol circulating in the blood is LDL. LDL contains only cholesterol esters and a type of apoproteins whose function is to transport cholesterol to peripheral tissues.

The LDL receptors that contain the cells in your skin are responsible for cholesterol uptake and the number of receptors depends on the amount of cholesterol they contain: higher cholesterol content, fewer receptors in the skin. Thus, when the cell has enough cholesterol, the LDL is still in the blood.
Based on epidemiological studies, it seems that maintaining a high level of LDL in blood increases the risk of arteriosclerosis and even infarction. Therefore, the bad cholesterol that these lipoproteins carry is called ‘bad cholesterol’.
On the other hand, high-density lipoproteins (HDL) are produced in the liver and in the intestine, and perform the reverse path, that is, they go from tissues to the liver. Its function is to collect the cholesterol that breaks the cells and bring it to the liver. It has been observed that the high level of HDL reduces the risk of arteriosclerosis, so the cholesterol associated with HDL is called “good cholesterol”.
Cholesterol guilty of arteriosclerosis
Although they differ between good and bad cholesterol, it is still not entirely clear to what extent the cholesterol that is ingested through food influences arteriosclerosis.

Arteriosclerosis is a chronic vascular disease that begins with small lesions of the blood vessels. The causes of lesions can be physical or chemical (high pressure, tobacco substances, etc. ). In any case, the lesion is closed by the accumulation of platelets in the inner layer of the arteries. In turn, there is inflammation that accumulates substances such as calcium soaps, phosphates, elastic fibers, collagen and bone components. But above all oxidized LDL are accumulated trapped by macrophages located on the wall of the tube. This process produces thickening and hardening of the arteries that can close the tube in the long term.
Although in the genesis of arteriosclerosis many other agents participate, for a long time it was considered that the cholesterol that is ingested along with food is one of the main agents.
In fact, the cholesterol introduced externally influences the amount of cholesterol that the body produces, that is, exogenous cholesterol can alter the endogenous cycle. When the cell takes cholesterol, the internal production stops, since the activity of the enzyme B-hydroxymethylglytaril CoA reductase is limited. On the other hand, LDL receptors disappear from the skin. These mechanisms are genetically controlled, but in some people the production of endogenous cholesterol is not stopped, nor is much exogenous cholesterol ingested. Therefore, they have high levels of cholesterol and LDL in the blood, which increases the risk of arteriosclerosis.

However, in later studies it has been shown that saturated fats are as important as the cholesterol that is taken, since they increase the levels of LDL. Also, to prevent arteriosclerosis, the best is the Mediterranean intake rich in unsaturated fats. Apparently, the oleic acid present in olive oil raises the level of HDL in blood, that is, it exerts a protective effect on the arteriosclerosis.
However, many agents are involved in arteriosclerosis (genetics, age, sex, obesity, physical exercise, smoking, diabetes...) and it must be taken into account that taking care of food is not always enough to prevent the disease. As on other occasions, the best way to escape is through a healthy lifestyle.
External cholesterol cycles captured and produced internally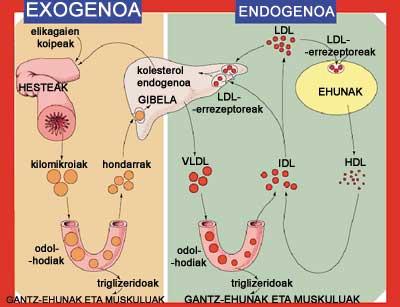
Drugs to reduce cholesterol
Sometimes, a healthy lifestyle, an adequate diet, and physical exercise are insufficient to reduce blood cholesterol and LDL levels. It is possible that by optional prescription the administration of drugs is necessary, especially in those cases where there is another factor that increases the risk of arteriosclerosis.

Some of these drugs prevent the accumulation of LDL in the wall of the blood vessels and the release of the clots. However, the most used are statins. With them the production of endogenous cholesterol is avoided, since they inhibit the enzyme B-hydroxymethylglytaril CoA, essential in the synthesis. Among them is cystastatin, which is sold under the name of Lipobay or Baycil and which last year was removed from the market because some patients suffered rhabdomyolysis and several deaths. However, if taken following the doctor's instructions, statins are beneficial, as they are able to reduce LDL in blood by 40%.
Other medications are associated with bile acids, which forces the liver to produce more bile acid, for which cholesterol is used, which reduces blood.
In addition, other drugs work lowering triglyceride levels or raising HDL levels. It seems that vitamin niacin also influences high doses. And, undoubtedly, the pharmaceutical industry will continue to investigate the drugs that so many people occupy in developed countries.
Influence of dietary ingredients on cholesterol and lipoproteins in blood| Ingredients of food | LDL and cholesterol | Triglycerides | HDL |
| Fat fat Fat Fat | |||
| Cholesterol Cholesterol Cholesterol Cholesterol | = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = = | ||
| Saturated fatty acids | |||
| Monounsaturated fatty acids | Ø Ø Ø | o o o o o o o o | |
| Polyunsaturated fatty acids | Ø Ø Ø | Ø Ø Ø | = or Ø |
| Excess of calories | Ø Ø Ø |
Buletina
Bidali zure helbide elektronikoa eta jaso asteroko buletina zure sarrera-ontzian







